Abstract:
Analysis of 703 MS patients showed that 300 HBO treatments (about
one treatment a fortnight over 10 - 13 years) appreciably arrested
progression of MS. More than 500 treatments, (approximately once per
week) are most effective. Patients who begin HBO treatment in the
early stages or with low initial initial Kurtzke values did best.
This Report follows the progress of many patients since they started
treatment over 10 years previously at the Multiple Sclerosis
National Therapy Centres in the UK. Hyperbaric Oxygen Therapy(HBOT)
was administered for treatment of Multiple Sclerosis.
MS National acknowledges the advice, guidance and support of its
Medical Advisors on Hyperbaric Medicine, Dr David Perrins, MD, FRCS
and Prof. Philip James, PhD, FFOM and this long-term study on the
effect of high dosage oxygenation on the course of MS.
In accordance with Title 17 U.S.C. Section 107, this material is
distributed without profit to those who have expressed a prior
interest in receiving the included information for research and
educational purposes.
Multiple Sclerosis is a disease of the nervous system that results
in localised patches of inflammation in the brain and spinal cord
which may eventually scar (sclerosis).
In 1983 the New England Journal of Medicine reported a controlled,
double-blind study on the effect of hyperbaric oxygenation on the
symptoms of multiple sclerosis. It reported scientifically
demonstrated benefits but recognised the need for long-term studies.
After a pilot study had confirmed this report, patients and their
relatives installed pressure chambers in 56 Centres throughout the
UK. Since 1982 over 12,000 UK patients have received HBOT. In most,
an initial intensive course has been followed by intermittent
maintenance treatment. Well over a million individual sessions have
been completed without untoward incident.
It is difficult to assess the effect of any treatment on MS patients
because of the unpredictable fluctuation of signs and symptoms. One
authority considers that the best experimental design is to observe
a large number of patients treated over a period of time. MS
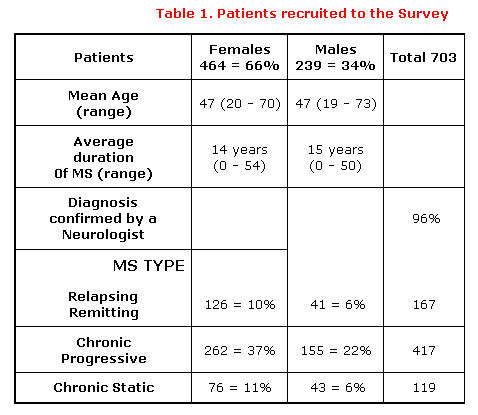
National therefore followed the progress of 703 patients who had
first received treatment soon after the centres opened.
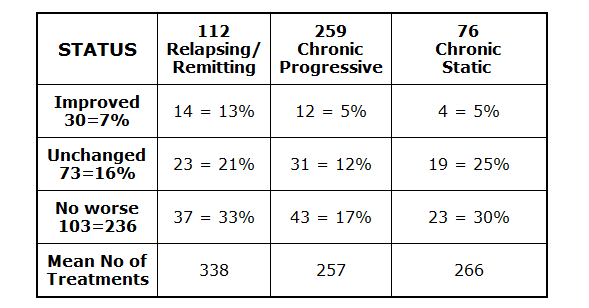
They were recruited from those attending 28 of the Centres. Details
are given in Table 1.
Patients had been told that they had multiple sclerosis by
neurologists who had said that there is no effective treatment for
their condition. The co-operation of the patient’s family doctor had
been obtained before they were accepted for treatment.
During HBO treatments, patients breathed 100% oxygen under pressure
in HBO chambers. The initial course of treatment consisted of twenty
sessions in 4 weeks. Thereafter, the patients returned for a
‘follow-on’ treatment on a weekly basis, or failing that, as often
as they felt the need or found it possible.
Patient Assessment
They were interviewed and assessed immediately before, during and
immediately after the initial 20-treatment course. Patients were
classified as Relapsing/Remitting, Chronic Progressive or Chronic
Static and assigned a Kurtzke Disability value from a scale (KDS)
that enables patients from different Centres to be compared. Between
two and four years, and again between six and eight years after the
initial course, another assessment was made. A further review was
conducted after 10 or more years.
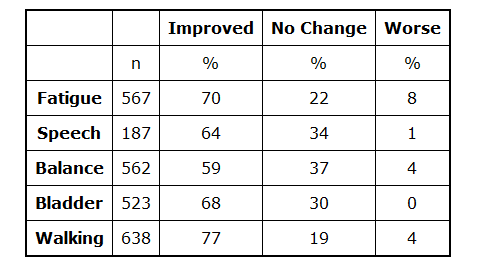
Twenty-five percent of Relapsing/Remitting patients improved on
their value, while 64 - 77% of symptoms improved (Table II).
Other improvements that significantly affect the quality of life
were gained during ttherapy, many of which were retained with
regular maintenance treatment in 73% of patients after 4 years.
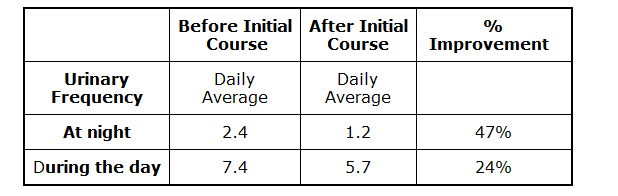
Subjective relief of bladder symptoms were confirmed by recording
urinary frequency (Table III).
Some patients complained that their symptoms were briefly made worse
- fatigue 20%, leg weakness 5%, visual disturbance 3% and limb
numbness 1%, but those symptoms were only short lived. Minor
problems with pressure on the eardrums occurred in 17%, but did not
necessitate stopping treatment.
Some patients lost their improvements within a week or two. Four
hundred and sixty-four patients (66%) who completed the initial
course continued with treatment for at least three years because
they found that their condition had stabilised, or the previous rate
of deterioration retarded. On the other hand, 239 patients (34%)
abandoned the treatment at intervals. Of these 25 later returned.
Thirty six patients (7 Relapsing/Remitting, 24 Chronic progressive
and 5 Chronic static) did not have any further treatment and after 6
years, 24 (67%) had deteriorated by a mean of 1.8 on the Kurtzke
scale.
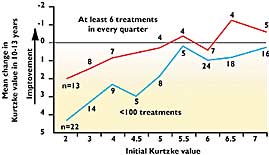
The rate of deterioration was inversely related to the frequency of
treatment. As might be expected, patients in the early stages of the
disease (Relapsing/Remitting) did best as there is less irreversible
damage in the nervous tissue. None of these (mean initial KDS 2.3)
who had received at least eight treatments in every quarter over 6
years had deteriorated. Indeed, four had actually improved by a mean
of 0.8 on the Kurtzke scale.
A third survey was conducted after 10 - 13 years. By then 126
patients had died (8% were over 60 years old when first treated), 99
were lost to follow up, 29 had suffered injuries that affected their
Kurtzke value and two had their diagnosis revised. Therefore 447
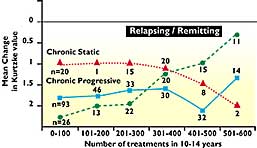
remained for analysis. The extent of deterioration clearly depends
on the frequency and duration of treatment (Figure 2).
Thirty eight of these patients had received less than 10 follow-on
treatments and had deteriorated by 3.18 on the KDS. It is therefore
evident that with an adequate dosage, progressive deterioration can
be retarded.
Table IV shows that 23% of the patients remaining eligible for
assessment were no worse after repeated treatments over 10 - 13
years. Even more remarkable are the 30 patients (7%) of patients who
have actually improved.
An analysis reveals that over 300 treatments (about one treatment a
fortnight over 10 - 13 years are required to appreciably arrest
progression and that more than 500 (say, once a week) are most
effective. Those patients with a low initial Kurtzke value do best
(Figure 3).
The natural history of MS is well established. Although there is a
wide variation in the rate and patterns of decline, the majority of
patients deteriorate over a two year period of observation. In this
series the Relapsing/Remitting patients who had less than two
follow-on treatments had deteriorated by 2.0 on the KDS after 10+
years, while the 31 who received more than 400 had only deteriorated
by 1.1. This represents a difference of being able to walk without
assistance and the need to use two sticks, or the ability to walk
200 yards and being confined to a wheel chair.
The Centres have attracted sufficient numbers of patients to allow
assessment of the effect of different dosage on different stages of
the disease. As might be expected, the response is better in
patients with less advanced disease. The treatment has been shown to
be safe, practicable, cost-effective and without side effects. After
10 or more years 38% of the 447 patients were still attending
regularly.
The findings imply that treatment with hyperbaric oxygen should be
instigated as soon as the condition is diagnosed and before
irreversible lesions have become established. The evidence suggests
that treatment should be given every week and may have to be
continued indefinitely.
Chambers
To Choose From
Click on
the Picture to Go To the Detailed Page
Free Shipping on all chambers w/in the USA
Balanced Health Today
355 Hukililke Street ( suite 206)
Kahului, Hi 96732
//www.BalancedHealthToday.com
info@BalancedHealthToday.com
888.449.0552





